Bone Regeneration Properties and Clinical Applications of Biphasic Calcium Sulfate- Case Study
Bone Regeneration Properties and Clinical Applications of Biphasic Calcium Sulfate
Amos Yahav, DMDa, Gregori M. Kurtzman, DDSb,*, Michael Katzap, DDSc, Damian Dudek, DDSd, David Baranes, DDSe
KEYWORDS
Calcium sulfate Biphasic calcium sulfate Graft Bone cements Sinus augmentation Socket preservation Ridge augmentation Osseous defect repair
KEY POINTS
Biphasic calcium sulfate has a complete conversion to host bone over a period of 4 to
6 months. The material sets hard, acting like a “bone cement” and has been used for decades in
orthopedics. Minimal flap reflection; flap closure is done under tension by stretching without releasing
incisions to induce a tension-free flap. No membrane is required, with primary closure not mandatory; when gaps in the soft tis- sue of 3 mm or less are present, the soft tissue migrates across to close the gap over a short period without inflammation. Various grafting applications are achievable with biphasic calcium sulfate at a more cost- effective material cost and similar clinical results can be achieved as with other grafting products used in dental surgery.
INTRODUCTION
Clinically, there are situations in dental treatment that require osseous grafting. Path- ologic voids (defects) or those surgically created during treatment may require grafting to restore the osseous anatomy. Conversely, resorption of the osseous contours may requiring grafting to place implants or augment around those implants to contain the entire implant within bone.
a Augma Biomaterials, Hadagan 15 Street, Katzir 37861, Israel; b Private Practice, 3801 Inter- national Drive, Suite 102, Silver Spring, MD 20906, USA; c Private Practice, 62-54 97th Pl, Rego Park, NY 11374, USA; d Artmedica Oral surgery department, Szosa Chelminska 166 street, Torun 87100 Poland; e Private Practice, Hatzadik Mishtefneshet 39 Street, Jerusalem 91000, Israel * Corresponding author. E-mail address: drimplants@aol.com
Dent Clin N Am 64 (2020) 453–472 https://doi.org/10.1016/j.cden.2019.12.006 dental.theclinics.com 0011-8532/20/© 2019 Elsevier Inc. All rights reserved.
Yahav et al 454
Various osseous grafting materials have been used clinically and reported in dental surgical applications. These include autografts, allografts, xenografts, and nonbiological-derived products (both synthetic and mineral based). Osseous grafts essentially act as a scaffold, maintaining the volume while allowing native bone forma- tion over time. Some materials will resorb fully, whereas others never fully resorb. Au- tografts and allografts will resorb and, depending on mineralization and compaction if cortical, cancellous or a mixture resorbs quickly (cancellous) or takes longer (cortical). Xenografts, specifically bovine materials do not fully resorb and residual particles remain long term.1 Synthetic graft materials, depending on their chemistry, may be replaced by conversion to host bone or remain partially or fully. The goal of grafting is conversion to native host bone that has vascularity that will remain in the long term, restoring the area to function; thus, selection of the material to be used is impor- tant to achieve that goal.
With those goals in mind, calcium sulfate, a natural mineral and one of the oldest biomaterials, has been used as a bone void filler, binder, grafting material, and as a delivery vehicle for pharmacologic agents and growth factors for more than 120 years, having a longer history of clinical use than most currently available biomaterials.2 The material has been used in a wide range of clinical applications in orthopedic, plastic surgery, oncologic, and maxillofacial applications in the treatment of osseous voids and traumatic or inflammatory bone deficiencies. Calcium sulfate exists in 3 different forms; calcium sulfate anhydrate, calcium sulfate dehydrate, and calcium sulfate hemihydrate. The difference between these chemical species is represented by the amount of water molecules residing within a single molecule unit. The crystalline struc- ture defines its physical, mechanical, and dissolution properties. The hemihydrate state of hydration exists as either an a or a b form, both of which are found in medical-grade calcium sulfate products. When this hemihydrate is mixed with water, a dehydrate is formed in a mild exothermic reaction with crystallization taking place, and the material sets and hardens.3 Calcium sulfate as an augmentation material was first reported by Dressman in 1892 to obliterate bone cavities caused by tubercu- losis.4 Later, in the 1920s and 1930s, Nystrom,5 and Edberg6 reported results on the use of calcium sulfate plaster of Paris as bone filler without any reported postoperative complications. An extensive review in 1966 regarding the use of calcium sulfate re- ported the material as a simple, inexpensive substance that offers many advantages as a graft material for bone filling.7 Studies have demonstrated that calcium sulfate is resorbable and is well tolerated by the tissues, acting primarily as a space filler, restoring morphologic contour, and preventing soft tissue ingrowth into the defects during the healing phase.8,9 Peltier and colleagues10–12 confirmed the osteoconduc- tive properties of calcium sulfate allowing ingrowth of blood vessels (angiogensis) and osteogenic cells. When calcium sulfate is implanted in the body, over time (short term) it completely dissolves leaving behind calcium phosphate deposits that stimu- late bone growth.13,14 Evidence has been reported that biphasic calcium sulfate not only serves as a 3-dimensional scaffold but also is able to promote osteoinduction.15 Therefore, it is considered a bioactive material.
A study reported 26 patients who had been treated with calcium sulfate for unicam- eral bone cysts, with a follow-up of 1 to 20 years. Of the study participants, 24 had successful healing of the defect with bone formation in the cyst, without complications or the need for additional surgery.16 Another study reporting on 110 patients treated with calcium sulfate, primarily for osseous defects in the skull and facial bones, concluded that calcium sulfate was an outstanding bone graft substitute that ensured bone formation and produced results comparable with, if not better than, autogenous bone graft.17 Extensive research has accumulated during the past few decades
Biphasic Calcium Sulphate Bone Regeneration 455
confirming the effective and safe use of calcium sulfate in both orthopedic and dental applications, consistently reporting high biocompatibility. In dental (maxillofacial and periodontal) applications, calcium sulfate has been used in a variety of clinical appli- cations, including periodontal defect repair, the treatment of osteomyelitis, radicular cyst defect repair, sinus augmentation, socket preservation, ridge augmentation, and as an adjunct to dental implant placement.18,19 Following graft placement, it can be monitored radiologically; during its placement, it appears radiopaque, after 2 to 3 weeks it appears radiolucent, and it regains radiopacity after 12 weeks, reflecting the transformation of the material into newly formed uncalcified osteoid turning grad- ually to calcified young native bone.
Following placement, during the healing phase, calcium sulfate dissolves into its component elements naturally found in the body. When placed in direct contact with viable host bone, new bone growth occurs in apposition to the calcium of the graft material. Calcium sulfate bioresorption studies and clinical experience have shown consistent osteoconduction and complete resorption, replaced by newly formed bone that is ultimately remodeled.20 Calcium ions activate platelets to release bone morphogenetic proteins and platelet-derived growth factors that stimulate prolifera- tion and osteogenic differentiation of mesenchymal stem cells.21,22 This makes this osseous graft material well tolerated and nonimmunogenic, with no adverse reactions or failure to heal being reported in the literature.23,24
Biphasic calcium sulfate acts as a cement, and its hard structure after fast setting prevents infiltration of epithelio-conjunctive cells into the material, acting as a barrier membrane. Yet, connective cells are able to proliferate over the surface of the ma- terial, promoting rapid healing of the overlaying soft tissue. Therefore, its related sur- gical protocols are less invasive compared with other grafting materials in which a tension-free flap and primary closure are mandatory. The opposite is found with biphasic calcium sulfate surgical protocols, indicating minimal flap reflection, and flap closure is done under tension with no releasing incisions to induce a tension- free flap,25 taking advantage of the flexibility of the mobile mucosa to stretch the flap into place for closure. Thus, the flap and graft are not influenced by muscle movements during the healing phase. In addition, maximal closure with graft expo- sure of 3 mm is acceptable. The hardness and stability of the biphasic calcium sul- fate placed into the defect being grafted means that no membrane or other intermediary barrier is needed. Biphasic calcium sulfate graft material has been shown not to compromise the desired results. Soft tissue cells at the flap margin pro- liferate over the exposed hardened graft, closing the flap margin fairly quickly over a few days to a week or so.
Calcium sulfate is considered to be one of the bone graft materials of choice in or- thopedics due to its excellent osteoconductive bioactivity capacity.26,27 It can be concluded that calcium sulfate is a biocompatible osteoconductive bioactive material that is well tolerated by the tissues when used for the treatment of osseous defects and guided tissue regeneration in animals and humans.
BIPHASIC CALCIUM SULFATE
In maxillofacial applications, however, difficulties with hardening calcium sulfate in the presence of saliva and bleeding have hampered its routine use. This obstacle to its use dentally was overcome in 2010 by Dr Amos Yahav by modifying the material behavior without changing its chemical structure or adding any additives making it biphasic. The biphasic calcium sulfate form allows the calcium sulfate to harden in the presence of saliva and blood, expanding its use in the maxillofacial arena. As
Yahav et al 456

Fig. 1. HA consists of particles of different sizes and shapes incorporated within the biphasic calcium sulfate matrix (scanning electron microscopy).
calcium sulfate is a completely resorbable synthetic material with short-term space- maintaining abilities, in the case of large osseous defects, the use of biphasic cal- cium sulfate as a composite graft in a mixture slows the resorption time allowing space maintenance, and the host replaces it with early bone. This is available as an already-made composite graft product called Bond Apatite (Augma Biomaterials), a biphasic calcium sulfate composite bone graft cement containing an average of one-third hydroxyapatite in a controlled particle distribution. The hydroxyapatite par- ticles are of various sizes and shapes of 90 mm to 1 mm (Fig. 1). On setting, the

Fig. 2. Postsetting structure of biphasic calcium sulfate at higher magnification, which is composed of needle-like crystals presenting microporosity (1–50 mm) and macroporosity (300–800 mm) promoting growth factor infiltration angiogenesis formation and cell prolif- eration (scanning electron microscopy).
material has a needle-like crystal structure (Fig. 2). This allows maintenance of the material in the defect for a much longer period, as the calcium sulfate component re- sorbs first, with later (slower) resorption of the hydroxyapatite component. This al- lows space maintenance of the defect while the host vascularizes the grafted area and develops bone, preventing soft tissue ingrowth. The cement has 2 resorption pattern mechanisms related to its components. The biphasic calcium sulfate portion has a resorption pattern of 4 to 10 weeks, which enables fast bone modeling and angiogenesis formation between the hydroxyapatite (HA) particles that act as a longer space maintainer to slow down the overall resorption of the graft. The small to middle-sized HA particles resorb completely after 3 to 5 months, then the larger particles, which are less than 10% by volume, remain for a longer period until com- plete resorption takes place. The resorption mechanism of the HA particles within the Bond Apatite cement is unique; the HA particles do not integrate with the newly formed bone. Instead, they become encapsulated by connective tissue where degradation occurs as the connective tissue undergoes ossification into a vital host bone.
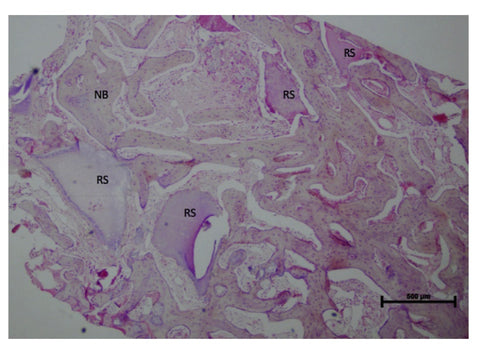
Histologically, in samples taken at 3 months after graft placement, new bone can be observed in close approximation to remaining residual scaffold particles of Bond Apatite (Fig. 3). Analysis at this stage of healing demonstrates w10% of residual graft particles surrounded by connective tissue. At 8 months after graft placement, histologically, little remains of the Bond Apatite and bone marrow is noted in the organizing new bone (Fig. 4). Some areas of connective tissue are also noted, indi- cating that the graft is maturing and the host is converting the graft material into native bone without any observed inflammatory process. Analysis at 8 months demonstrates the components of the sample to be 79% bone, 11% bone marrow, 7% connective tissue, and only 3% residual graft particles.
Bond Apatite is provided in a double-compartment syringe with one side con- taining the composite mixture of biphasic calcium sulfate powder with hydroxyap- atite and the other compartment containing sterile saline solution. Advancing the syringe shaft until the first plunger on the syringe reaches the blue line marked on the syringe activates the material. The syringe cap is then removed, and the graft is ready for placement directly into the osseous defect. After placement into the defect, sterile gauze is pressed firmly over the graft for 3 seconds to remove residual moisture and harden the material, while compressing it to the
Biphasic Calcium Sulphate Bone Regeneration 457
Fig. 3. Histology of Bond Apatite graft specimen at 3 months after graft placement showing residual graft scaffold (RS) and new bone (NB) within the sample studied.
Yahav et al 458


Fig. 4. Histology of Bond Apatite graft specimen at 8 months after graft placement showing (right) bone (purple), bone marrow (blue), connective tissue (green), and residual graft par- ticles (yellow).
osseous bed. Soft tissue is then reapproximated by stretching, and sutures are placed to fixate the flap margins. The flap should be positioned in direct contact with the graft with tension and secured with sutures. A membrane is not required between the graft material and soft tissue. Exposure of the graft material of up to 3 mm does not require membrane coverage or mobilization of the soft tissue to achieve primary closure. Because of the biocompatible nature of the biphasic cal- cium sulfate and its set hardness, any minimal exposure will result in peripheral soft tissue migration to cover the material without loss of graft material in the interim period.
As a salt, the graft material has bacteriostatic qualities, which are induced by the presence of sodium chloride in the physiologic saline used to mix the powder with the liquid.28 The cement obtained after mixing the biphasic calcium sulfate powder with the physiologic saline has bonding qualities. After mixing, it is deposited into the osseous defect in a dehydrated (wet) form. The material is then compressed with sterile gauze for 3 seconds to remove any residual liquid, resulting in a dehy- drated crystallized form, which hardens and sticks to the osseous defect walls, thus forming a stable block unlike graft materials in granule or paste form. Bond Apatite may be used in small and large defects, such as socket grafting, periodontal defects, lateral ridge widening, and horizontal sinus augmentation (crestal and lateral approaches).
CLINICAL APPLICATIONS Extraction Socket Preservation (Grafting)
Extraction socket grafting is often indicated to preserve the osseous crestal margins and prevent resorption during healing (Fig. 5). This may also be performed in anticipation of implant placement at a later date or simultaneous with the extraction. After extraction, the sockets are thoroughly curetted to remove any residual tissue or pathologic matter. Bond Apatite is mixed and placed into the extraction socket by injection from the syringe. It is not necessary to place a membrane over the graft material. However, exposure of several millimeters (>3 mm) of set material at the superior aspect of the crest requires a simple collagen sponge with average resorption of 7 to 10 days, which should be secured in place to cover and protect the exposed material during the first healing stage until soft tissue proliferation takes place above its surface; this does not affect the clinical results. Sutures are placed to help maintain the soft tissue margins with the collagen sponge in contact with the graft material during initial healing (Fig. 6). After 4 months

Fig. 5. Radiograph demonstrating failure of bridge abutments related to endodontic failure and periodontal bone loss.

Fig. 6. After extraction of the bridge abutment teeth, the extraction sockets were curetted and filled with Bond Apatite, and exposed material over 3 mm was covered by a collagen sponge secured in place by sutures to help contain the graft material without primary closure of the soft tissue.

Fig. 7. Presentation at 4 months after surgery demonstrating complete coverage of the area with keratinized soft tissue and closure of the areas of Bond Apatite that had been left exposed at completion of the surgical appointment.
Yahav et al 460

Fig. 8. Radiograph at 4 months after surgical placement of Bond Apatite demonstrating early bone fill and conversion of the graft material.

Fig. 9. Site was flapped at 4 months after surgical grafting demonstrating bone filling the extraction sockets previously grafted.

Fig. 10. Core sample retrieved with a trephine from a surgical site that had been grafted with Bond Apatite 4 months previously.

Fig. 11. Radiograph after implant placement at 4 months and socket grafting with Bond Apatite.


Fig. 12. Histologic evaluation of the core specimen at 40Â demonstrating residual particles of Bond Apatite (yellow, right side) and young bone in proximity with the particles.
Biphasic Calcium Sulphate Bone Regeneration 461


Fig. 13. Microscopic evaluation of the core specimen at 200Â demonstrating residual parti- cles of Bond Apatite (yellow, right side) and young bone (blue, right side) in proximity with the particles.
Yahav et al 462

Fig. 14. Periapical radiograph with a lesion associated with previous endodontic treatment on the left mandibular lateral and central incisors.

Fig. 15. Cone beam computed tomography cross-section demonstrating the size of the odontogenic cyst associated with failing endodontic teeth in the mandibular anterior, with lack of facial plate noted.
Biphasic Calcium Sulphate Bone Regeneration 463

Fig. 16. Size of the defect after enucleation of the odontogenic cyst, root resection, and retrograde filling.
of site healing, the previously exposed areas at the superior aspect of the crest are covered with keratinized gingiva (Fig. 7). A radiograph confirms osseous fill of the extrac- tion sockets (Fig. 8). The area is flapped for implant placement, demonstrating osseous fill of the sockets (Fig. 9), and a core sample is removed by trephine (Fig. 10). Implants are placed as planned and a radiograph is taken (Fig. 11). Histologic evaluation of the core specimen demonstrates residual particles of Bond Apatite with young bone in proximity with the few remaining particles (Figs. 12 and 13). The remaining graft particles will convert while the implants are integrating.
Radicular Cyst or Defect Grafting
An osseous defect resulting from pathologic lesions may necessitate surgical intervention to remove the source of the lesions (Figs. 14 and 15). The area is flap- ped and pathologic tissue is excised, leaving an osseous defect that will require grafting (Fig. 16). Bond Apatite is mixed and placed into the osseous defect until the graft material is flush with the exterior aspect of the ridge (Fig. 17). After a heal- ing period, radiographs are taken to verify conversion of the graft material placed into host bone (Figs. 18 and 19). Histologic analysis via a trephined core sample of the site demonstrates some residual particles of Bond Apatite with new young bone formulation with the absence of an inflammatory reaction (Fig. 20). Immuno- histochemical study (CD68, a surface antigen used for detection of bone cells)
Yahav et al 464

Fig. 17. Bond Apatite placement to fill a large osseous defect.
demonstrates active osteoblasts in the tissue and little remaining Bond Apatite (Fig. 21).
Sinus Elevation via a Crestal Approach
The osteotomy is prepared in anticipation for crestal sinus elevation. The sinus is elevated using Summers’ technique. Bond Apatite is activated in its syringe and then injected into a sterile dish and left to harden for 3 minutes. Thereafter, the semi-hard material is reloaded back into the Bond Apatite syringe barrel or any other bone graft carrier and introduced into the osteotomy (Fig. 22). An osteotome is used to gently place the graft material into the elevated sinus area (Fig. 23). When the implant can be placed at that appointment, it is introduced into the site, a cover screw placed, and the site closed with a suture across. Should an implant not be able to be placed at that appointment, the entire osteotomy is filled with additional Bond Apatite, compressed with gauze, and the site closed with a suture over the socket. After a period of 4 months to allow the sinus augmentation graft to heal, im- plants were placed in the new available crestal height and further healing was allowed for implant integration (Fig. 24).
Sinus Elevation via a Lateral Approach
Conventional preparation of the lateral window for sinus elevation is performed after flap elevation and the sinus membrane is elevated (Fig. 25). Bond Apatite

Fig. 18. Bond Apatite placement to fill a large osseous defect.
Biphasic Calcium Sulphate Bone Regeneration 465

Fig. 19. Cone beam computed tomography cross-section at 6 months demonstrating replacement of the Bond Apatite with new host bone maintaining the facial contour of the mandible cortical plate that was affected by the lesion that was removed.
Yahav et al 466

Fig. 20. Histology after 3 months, shown at 100Â with visible new young bone formulation (dark purple spots) and residual Bond Apatite (dark areas) that is converting to bone with the absence of an inflammatory reaction.

Fig. 21. Immunohistochemical study of CD68, a surface antigen used for detection of bone cells, demonstrates active osteoblasts in the tissue and little remaining Bond Apatite (green).

Fig. 22. Bond Apatite is introduced into the crestal sinus elevation with the syringe.

Fig. 23. An osteotome is used to compact the Bond Apatite graft material into the crestally elevated maxillary sinus before implant placement.

Fig. 24. After a healing period of 4 months to allow the sinus augmentation graft to heal, implants were placed in the new available crestal height and with further healing,allowed implant integration.
Biphasic Calcium Sulphate Bone Regeneration 467

Fig. 25. A lateral osseous window has been created in the posterior maxilla as a prelude to sinus augmentation.
Yahav et al 468

Fig. 26. Bond Apatite is mixed and a syringe is used to introduce the graft material into the elevated maxillary sinus.
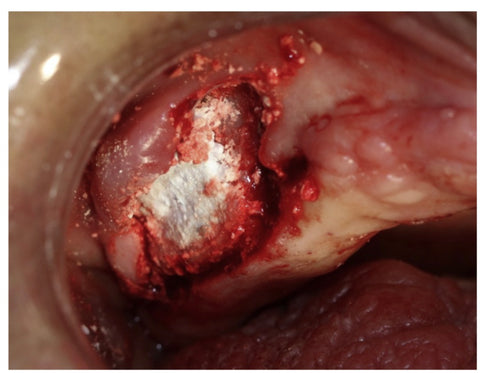
Fig. 27. The elevated maxillary sinus is filled with Bond Apatite graft material to the exterior contour of the lateral wall of the sinus.

Fig. 28. Posterior mandible with insufficient width to accommodate implants has had the buccal aspect of the ridge perforated to create bleeding points in preparation for graft placement.
is mixed and after a 1-minute waiting time, is injected into the sinus that was created by elevation of the sinus membrane (Fig. 26). The graft is dispersed in the sinus cavity first mesial, then distally, and finally in the center until two- thirds of the sinus is filled. During graft dispersion, the graft material should be compressed against the crest and the sinus walls and, if needed, dry sterile gauze is used to tap gently over the graft surface to absorb excess fluids and blood. When filling the last one-third and closing the sinus window, the last syringe of Bond Apatite is activated and immediately injected into the sinus, followed by pressing firmly for 3 seconds with dry sterile gauze. The augmen- tation is finished with graft material level with the buccal aspect of the bony window that was created (Fig. 27).
Lateral Ridge Grafting (Osseous Width Deficiency)
A full thickness flap extended 2 to 3 mm past the mucogingival line is reflected to visualize the site. If the crestal incision is long enough in the mesial distal di- rection, a vertical releasing incision may not be necessary and an envelope technique may be used. Decortication with a surgical carbide in a handpiece is performed on the buccal aspect of the ridge. This aids in providing stem cells for the graft to be placed (Fig. 28). Bond Apatite is activated in the syringe and placed over the buccal lateral aspect of the ridge, then compressed with gauze
Biphasic Calcium Sulphate Bone Regeneration 469

Fig. 29. The lateral aspect of the ridge has been grafted with Bond Apatite before flap closure.
Yahav et al 470

Fig. 30. The flap has been reapproximated over the graft and secured with sutures.
for 3 seconds (Fig. 29). The flap is repositioned directly on the graft under ten- sion by stretching it for maximal closure over the graft. If primary closure cannot be achieved, 3 mm of graft exposure is acceptable and a membrane is not required to cover any of the exposed graft material. Sutures are placed to fixate the soft tissue (Fig. 30). After a 3- to 4-month healing period, the site is reflap- ped for implant placement, demonstrating ridge width that can accommodate
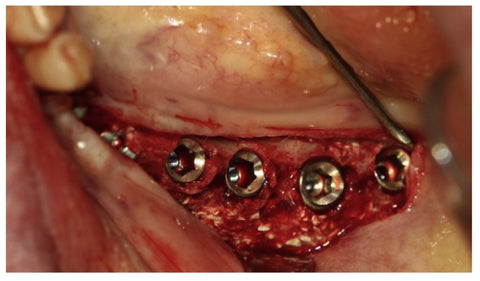
Fig. 31. At 3 months after grafting surgery, implants have been placed in the wider resulting ridge, with some particles of the Bond Apatite remaining that will finish conversion while the implants integrate.
Biphasic Calcium Sulphate Bone Regeneration 471
the planned implants (Fig. 31). Residual graft particles may be noted at this phase and will fully convert as the implants integrate.
SUMMARY
The goal of osseous grafting is to maintain a space to provide a scaffold for the host to peripherally accomplish angiogenesis and replace the graft by host bone. To accom- plish this, the graft material needs to be biocompatible and resorbable over time, but remain long enough to allow host conversion. Biphasic calcium sulfate provides a graft material with a long history in both orthopedic and maxillofacial applications. The addi- tion of HA increases the resorption time and remains within the practical time frame for dental clinical applications with most of the graft material converting to young bone in a 3- to 6-month period and the remainder resorbing shortly thereafter. As outlined, these applications include elimination of osseous defects created either pathologically or as a result of surgical treatment and those clinical situations where osseous devel- opment is a prelude to implant treatment.
REFERENCES
- Ohayon L. Histological and histomorphometric evaluation of anorganic bovine bone used for maxillary sinus floor augmentation: a six-month and five-year follow-up of one clinical case. Implant Dent 2014;23(3):239–44. 2. Thomas MV, Puleo DA. Calcium sulfate: properties and clinical applications.
J Biomed Mater Res B Appl Biomater 2009;88(2):597–610. 3. Thomas MV, Puleo DA, Al-Sabbagh M. Calcium sulfate: a review. J Long Term Eff
Med Implants 2005;15(6):599–607. 4. Dreesman H. Ueber knochenplombierung. Beitr Klin Chir 1892;9:804. 5. Nystrom G. Plugging of bone cavities with rivanol-plaster-porridge. Acta Chir
Scand 1928;63:296. 6. Edberg E. Some experiences of filling osseous, cavities with plaster. Acta Chir
Scand 1930;67:313–9. 7. Bahn SL. Plaster: a bone substitute. Oral Surg Oral Med Oral Pathol 1966;21(5):
672–81. 8. Pecora G, Andreana S, Margarone JE 3rd, et al. Bone regeneration with a cal- cium sulfate barrier. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997; 84(4):424–9. 9. Kim CK, Kim HY, Chai JK, et al. Effect of a calcium sulfate implant with calcium sulfate barrier on periodontal healing in 3-wall intrabony defects in dogs. J Periodontol 1998;69(9):982–8. 10. Peltier LF, Bickel EY, Lillo R, et al. The use of plaster of paris to fill defects in bone.
Ann Surg 1957;146(1):61–9. 11. Peltier LF. The use of plaster of paris to fill large defects in bone. Am J Surg 1959;
97(3):311–5. 12. Peltier LF. The use of plaster of Paris to fill defects in bone. Clin Orthop 1961;
21:1–31. 13. Yuan W, He X, Zhang J, et al. Calcium phosphate silicate and calcium silicate ce- ments suppressing osteoclasts activity through cytokine regulation. J Nanosci Nanotechnol 2018;18(10):6799–804. 14. Urquia Edreira ER, Hayrapetyan A, Wolke JG, et al. Effect of calcium phosphate ceramic substrate geometry on mesenchymal stromal cell organization and oste- ogenic differentiation. Biofabrication 2016;8(2):025006.
Yahav et al 472
- Raina DB, Gupta A, Petersen MM, et al. Muscle as an osteoinductive niche for local bone formation with the use of a biphasic calcium sulphate/hydroxyapatite biomaterial. Bone Joint Res 2016;5(10):500–11. 16. Peltier LF, Jones RH. Treatment of unicameral bone cysts by curettage and pack-
ing with plaster-of-Paris pellets. J Bone Joint Surg Am 1978;60(6):820–2. 17. Coetzee AS. Regeneration of bone in the presence of calcium sulfate. Arch Oto-
laryngol 1980;106(7):405–9. 18. Strocchi R, Orsini G, Iezzi G, et al. Bone regeneration with calcium sulfate: evi- dence for increased angiogenesis in rabbits. J Oral Implantol 2002;28(6):273–8. 19. Intini G, Andreana S, Margarone JE 3rd, et al. Engineering a bioactive matrix by
modifications of calcium sulfate. Tissue Eng 2002;8(6):997–1008. 20. Bagoff R, Mamidwar S, Chesnoiu-Matei I, et al. Socket preservation and sinus augmentation using a medical grade calcium sulfate hemihydrate and mineral- ized irradiated cancellous bone allograft composite. J Oral Implantol 2013; 39(3):363–71. 21. Huang TH, Kao CT, Shen YF, et al. Substitutions of strontium in bioactive calcium silicate bone cements stimulate osteogenic differentiation in human mesen- chymal stem cells. J Mater Sci Mater Med 2019;30(6):68. 22. Ali Akbari Ghavimi S, Allen BN, Stromsdorfer JL, et al. Calcium and phosphate ions as simple signaling molecules with versatile osteoinductivity. Biomed Mater 2018;13(5):055005. 23. Robinson D, Alk D, Sandbank J, et al. Inflammatory reactions associated with a
calcium sulfate bone substitute. Ann Transplant 1999;4(3–4):91–7. 24. Evaniew N, Tan V, Parasu N, et al. Use of a calcium sulfate-calcium phosphate synthetic bone graft composite in the surgical management of primary bone tu- mors. Orthopedics 2013;36(2):e216–22. 25. Baranes D, Kurtzman GM. Biphasic calcium sulfate as an alternative grafting ma-
terial in various dental applications. J Oral Implantol 2019;45(3):247–55. 26. Hak DJ. The use of osteoconductive bone graft substitutes in orthopaedic
trauma. J Am Acad Orthop Surg 2007;15(9):525–36. 27. Gitelis S, Piasecki P, Turner T, et al. Use of a calcium sulfate-based bone graft
substitute for benign bone lesions. Orthopedics 2001;24(2):162–6. 28. Nun ̃ez de Gonzalez MT, Keeton JT, Acuff GR, et al. Effectiveness of acidic cal- cium sulfate with propionic and lactic acid and lactates as postprocessing dip- ping solutions to control Listeria monocytogenes on frankfurters with or without potassium lactate and stored vacuum packaged at 4.5 degrees C. J Food Prot 2004;67(5):915–21.